Types of Breast Reconstruction
Getting through breast cancer treatment can be an overwhelming experience. And if you’re going to have a mastectomy or lumpectomy, it can be hard to decide if you want to have breast reconstruction — or which type to get.
Decisions about breast reconstruction are very personal, so take the time you need to figure out the best options for you. For some people, rebuilding the breasts is an important step that helps them move forward and feel more comfortable with their body after breast cancer. Others don’t feel the need for that extra step, or they prefer not to rebuild the breasts because they’d rather not get additional surgery. Some might choose a middle path and do a less invasive procedure that involves reshaping the breast by rearranging tissue but isn’t a full reconstruction.
There are several different breast reconstruction procedures that can restore the shape and appearance of one or both breasts after mastectomy. Among the most common are:
implant reconstruction: the breast is recreated with an implant
flap reconstruction: the breast is recreated with tissue from another part of the body
Goldilocks mastectomy: a small breast mound is created using remaining skin and fat
aesthetic flat closure, also known as “going flat”: the breasts are not rebuilt, but the appearance and contour of the chest is smoothed out
Some of the types of reconstruction that are done after a mastectomy can be combined with procedures that help restore sensation to the breast and nipples.
There are also several reconstruction procedures that can be used after lumpectomy, but one of the most common is:
oncoplastic surgery: the breast tissue is rearranged to replace lost volume; sometimes a lift or reduction on both breasts is also done
Most people who have a mastectomy or lumpectomy can get breast reconstruction. But not everyone is a candidate for all forms of breast reconstruction. Your options will depend on factors such as your anatomy, history of past surgeries, and whether you have other health conditions.
If you’re considering getting breast reconstruction surgery, it’s a good idea to meet with one or more board-certified plastic surgeons who specialize in breast reconstruction before you have a mastectomy or lumpectomy. They can help you understand your options.
Download the booklet Breast Reconstruction: A Guide to Your Options in English or Spanish, or order printed copies.

Implant reconstruction
Pros:
many options for size and shape of the reconstructed breast
shorter and simpler surgery than flap reconstruction, with a shorter hospital stay (1–2 days or less)
quicker recovery than flap reconstruction (4–6 weeks)
very common surgery that many plastic surgeons can do
Cons:
often requires multiple surgeries
requires more follow-up care, including regular checks for implant rupture
possible complications, like capsular contracture (tightening of scar tissue around the implant), breast implant illness, and rare cancers such as BIA-ALCL
implants don’t last a lifetime and they generally need to be removed and replaced about every 10–15 years
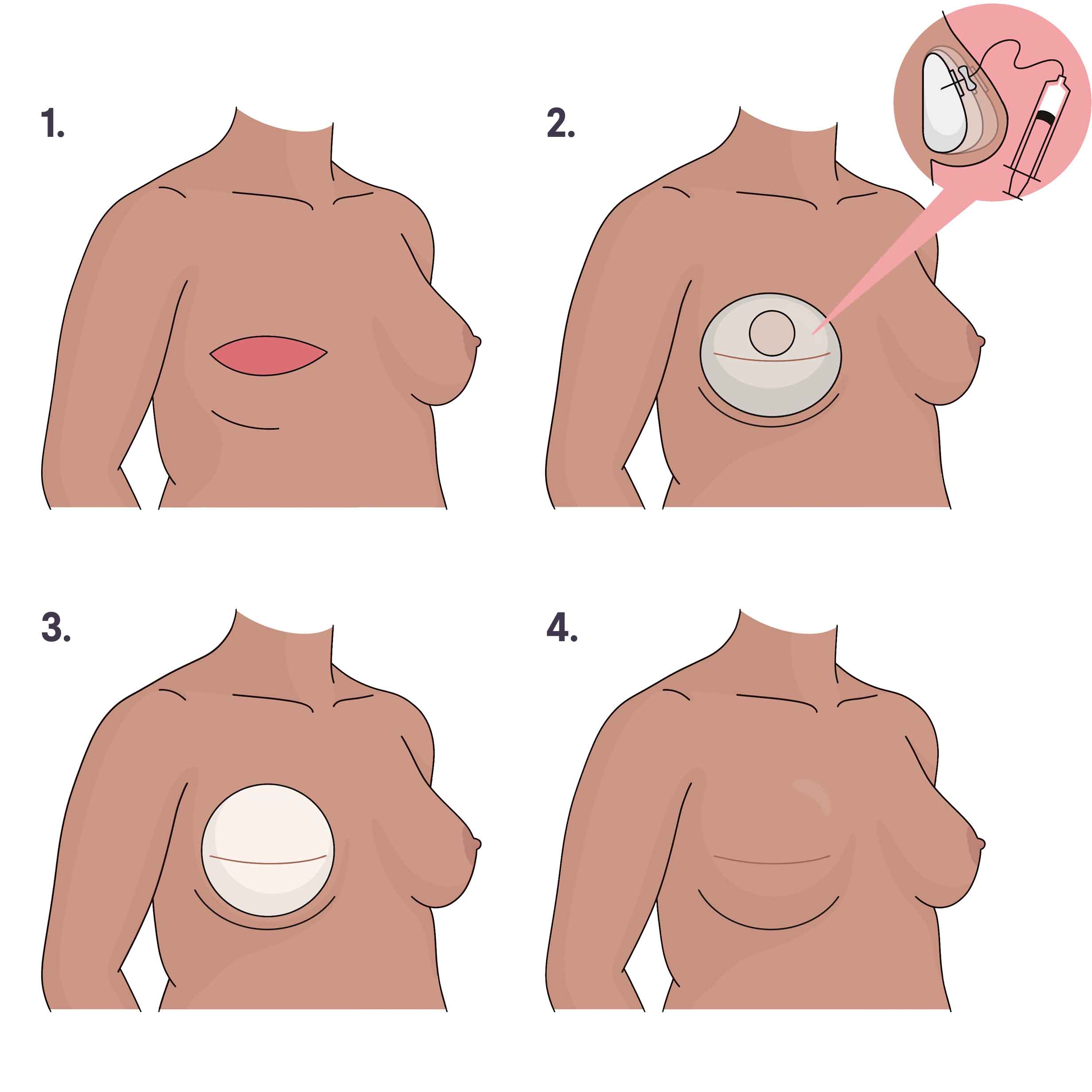
1. Breast tissue and nipple are removed. 2. A tissue expander is placed and gradually filled with sterile water over several weeks until it’s the preferred size. 3. The expander is exchanged for a permanent breast implant in a second surgery. 4. The breast, with implant, heals with a scar. Illustration by You Jeong (Julie) Park, MD.
How it’s done: Implant reconstruction uses an implant — a round, flexible silicone shell that’s filled with silicone gel or saline (salt water) — to restore the shape and volume of the breast. A breast implant can be placed either underneath part or all of the chest muscle (subpectoral or under the muscle) or on top of the chest muscle (prepectoral or over the muscle).
When it’s done: Some people can get implants in a single procedure at the same time as the mastectomy surgery. More commonly, though, implant reconstruction involves two or more surgeries over a three- to 12-month period. In the first stage, the surgeon places temporary breast implants called tissue expanders either under or on top of the chest muscle. Tissue expanders have a small valve that can be filled over time with salt water or air. They’re used to gradually stretch the skin and soft tissue to create a space that will hold the implant. For six to eight weeks, you’ll go for regular office visits so your plastic surgeon can fill the expander(s) until a desired size is reached. Then, you’ll have a second surgery to remove the tissue expander and replace it with a breast implant.
Who can get it: Most people are candidates for implant reconstruction, unless they have certain factors — like being a smoker or having prior radiation to the chest area — that put them at high risk of complications.
How long does it take: 1–2 hours per breast to place either a tissue expander or an implant.
DIEP flap and other flap reconstruction
Pros:
may have a more natural look and feel than implants
the reconstruction usually lasts a lifetime
lower risk of long-term complications
some people like that their stomach is flatter after the removal of abdominal tissue
Cons:
long and complex surgery
recovery time can be long (six to eight weeks or more) due to multiple surgical sites that need to heal
scars on multiple parts of the body
possible complications like flap necrosis (when part or all of the flap dies because it doesn’t get enough blood supply) and abdominal hernia or weakness
fewer plastic surgeons do flap reconstruction (and it might be harder to find one in your insurance plan’s network)
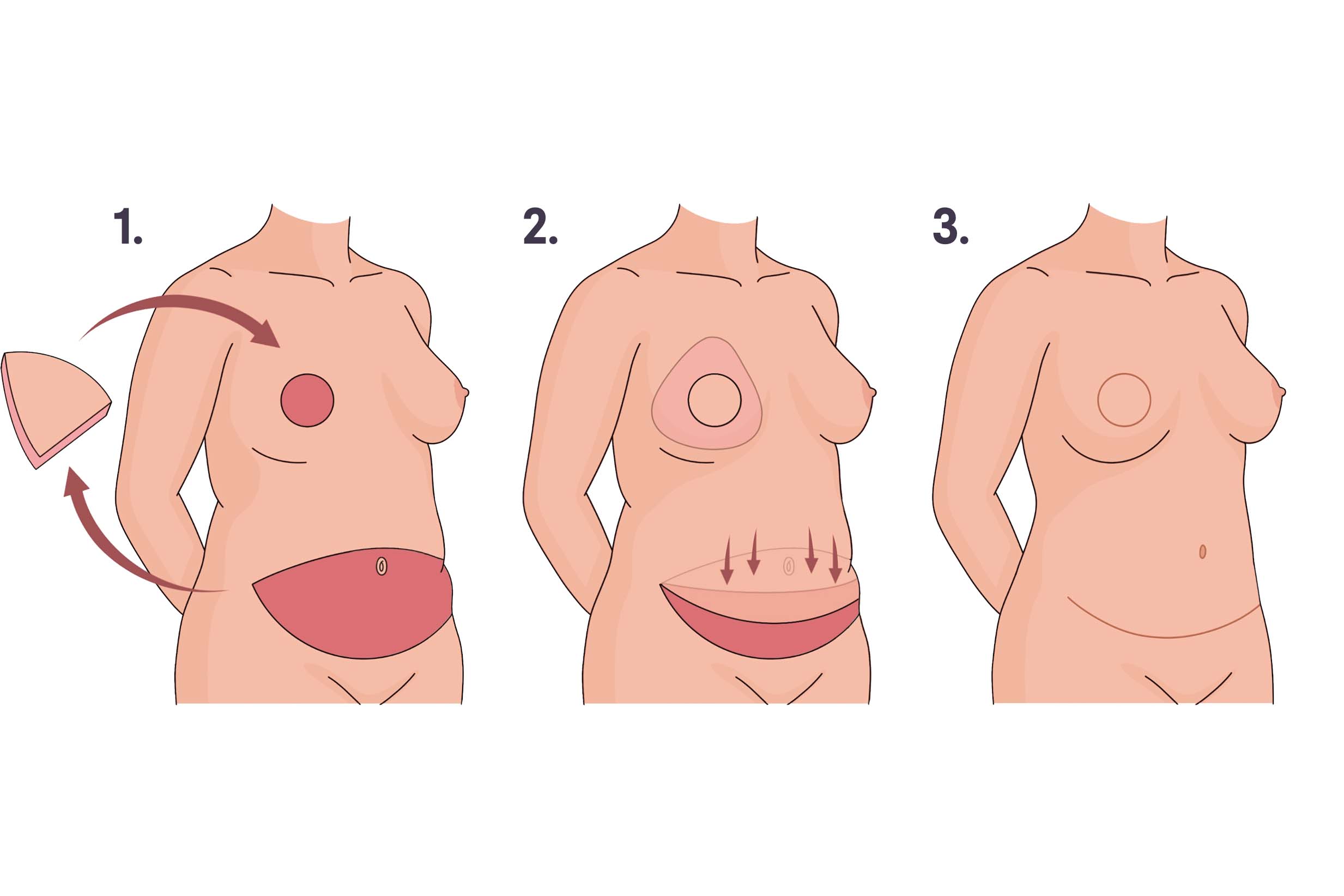
1. Breast tissue and nipple are removed and a flap of tissue is removed from the abdomen. 2. The flap is moved to the chest to create a breast mound, and blood vessels in the flap are connected to blood vessels in the chest. The abdominal skin is pulled down and the belly button is repositioned. 3. Incisions in the breast and abdomen are closed. Illustration by You Jeong (Julie) Park, MD.
How it’s done: Flap reconstruction (also called autologous breast reconstruction) uses a flap of tissue that’s removed from another place on the body and transferred to the chest to form a breast shape. The tissue flap includes skin, fat, blood vessels, and sometimes muscle. Using microsurgery, the surgeon connects the blood vessels in the flap to the blood vessels in the chest, creating a reconstructed breast with its own blood supply.
The most commonly done flap procedure is deep inferior epigastric perforator (DIEP flap) reconstruction. During DIEP flap surgery, a flap of tissue is removed from the lower belly (the area that is removed during a “tummy tuck”) and transferred to the chest to rebuild one or both breasts.
There are also several other types of flap procedures that use tissue from, for example, the back of the upper thigh, the lower back just above the buttocks, or other areas of the body.
When it’s done: At the same time as the mastectomy or as a separate procedure done weeks, months, or even years later. In some situations — if you’re going to have radiation therapy after a mastectomy, for example — your surgeon might suggest you get tissue expanders at the time of the mastectomy and then have flap reconstruction months later.
Who can get it: People who have enough tissue in the part of the body where the flap will be removed from (and haven’t had certain prior surgeries in that area of the body) and who are healthy enough to undergo a longer surgery are usually candidates for flap reconstruction.
If you don’t have enough fatty tissue in one area of the body to build a breast that’s the size you want, a surgeon might recommend hybrid flap/implant reconstruction (using a flap of your own tissue along with a small breast implant to rebuild the breast) or stacked flap reconstruction (using two or more tissue flaps to rebuild the breast).
How long does it take: 3–4 hours to rebuild one breast or 6–7 hours to rebuild both
Goldilocks mastectomy
Pros:
surgery is quicker and less invasive than flap or implant reconstruction
shorter recovery time
lower risk of certain complications
no implants or tissues from other parts of the body need to be used
Cons:
the reconstructed breast size is limited by the amount of tissue available; fewer options for size and shape of reconstructed breast
results are less predictable
the breast mound can flatten over time
fat necrosis is a common complication
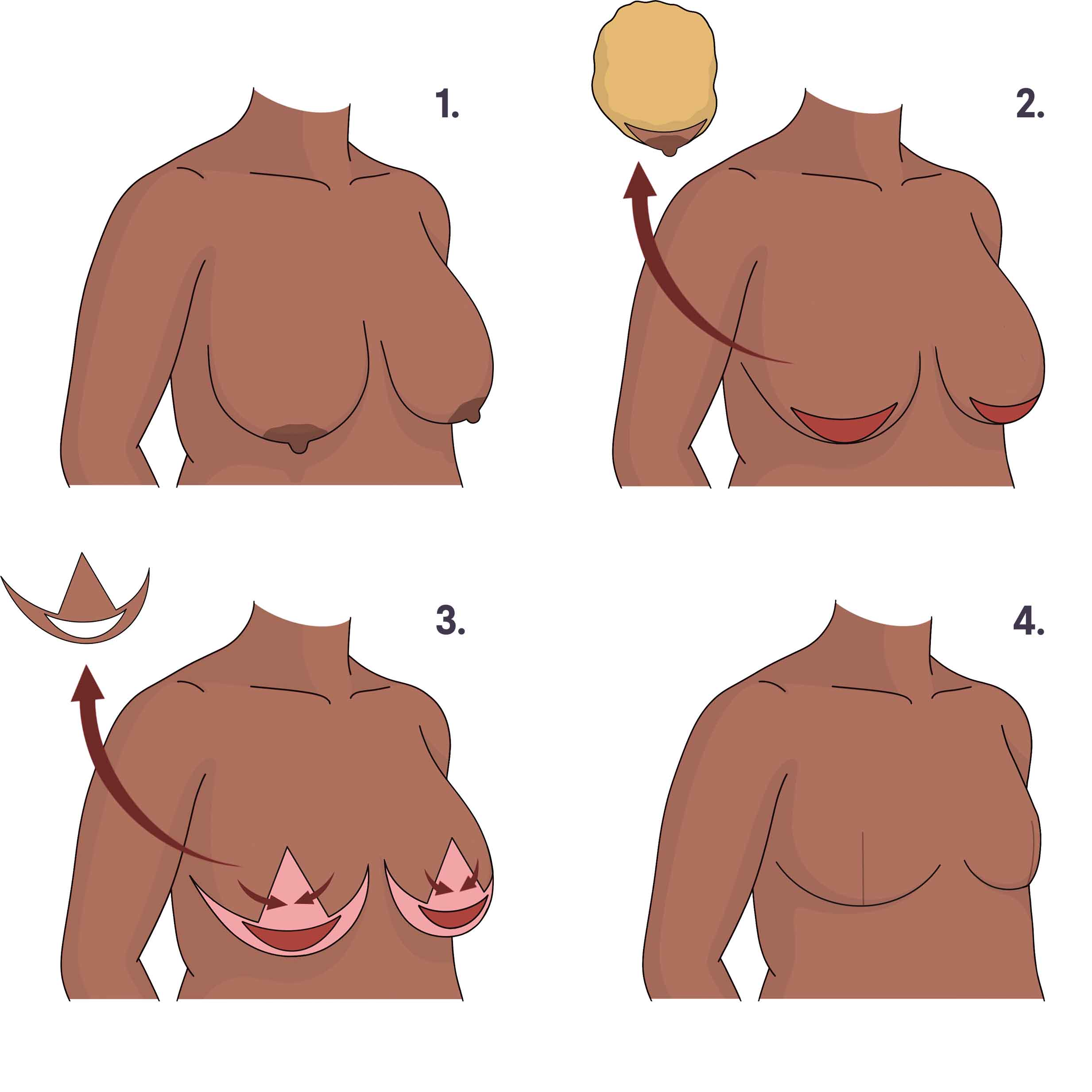
1. Breasts before surgery. 2. Breast tissue and nipples are removed. 3. An outer layer of skin is removed from the remaining breast skin. 4. Remaining skin and fat is rearranged to create small breast mounds, and incisions are closed. Illustration by You Jeong (Julie) Park, MD.
How and when it’s done: A Goldilocks procedure is done at the same time as the mastectomy, right after the breast tissue is removed. The surgeon uses the remaining fatty tissue and skin to form a new, smaller breast mound. Some people choose to have one or more fat grafting procedures later on to add volume to the reconstructed breast(s). This involves removing fat from another part of the body using liposuction and injecting it into the breast area. A nipple-sparing Goldilocks mastectomy is sometimes called a SWIM procedure.
Who can get it: The procedure works best for people with larger breasts or those with more of a droop (known as ptosis).
Length of surgery: 1.5–2 hours to rebuild one breast or 3 hours to rebuild both
Aesthetic flat closure (going flat)
Pros:
surgery is quicker and and less invasive than flap or implant reconstruction
shorter recovery time
lower risk of complications
no implants or tissues from other parts of the body are used
Cons:
some people may not like having a flat chest (or having a flat chest on one side).
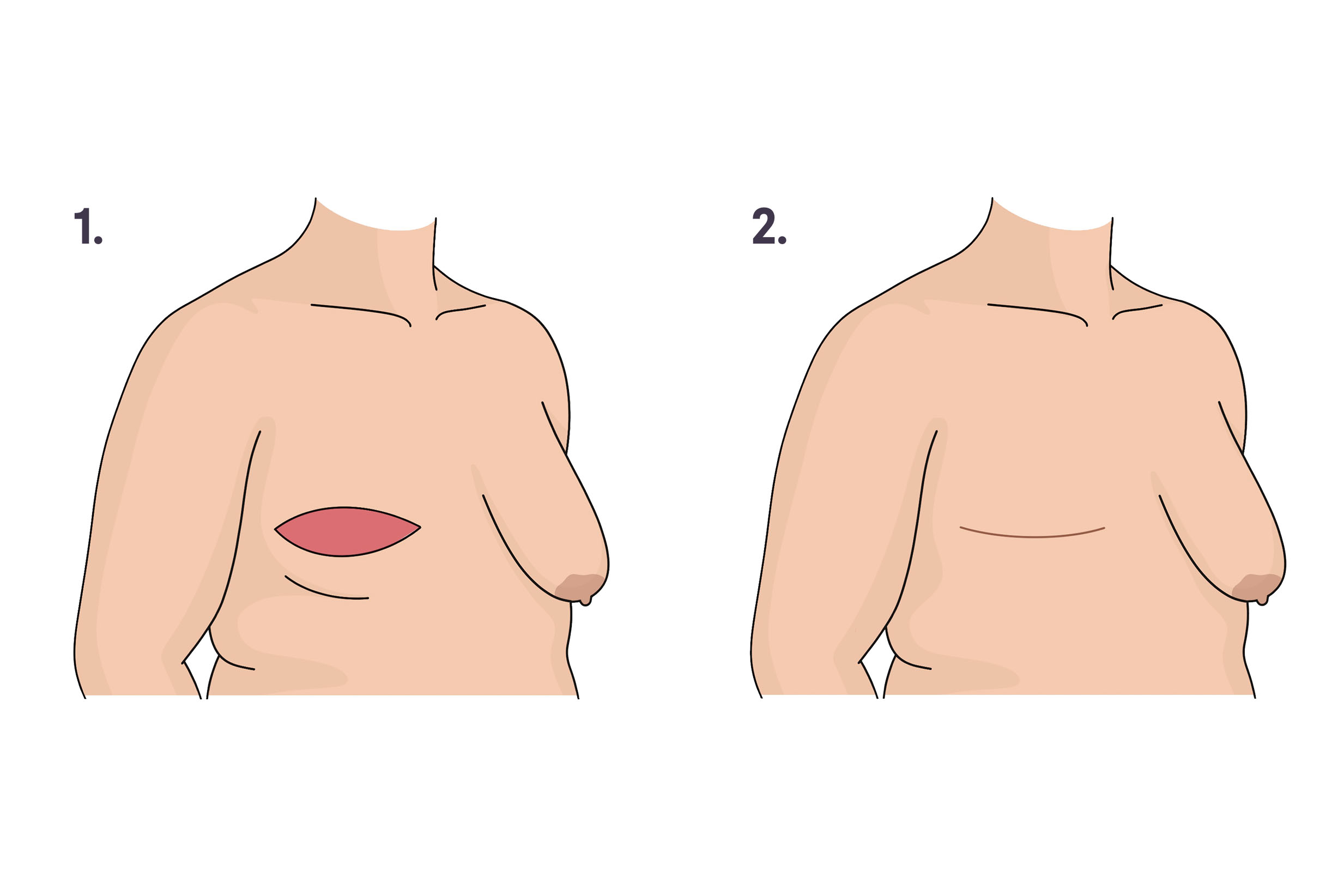
1. Breast tissue, nipple, and extra skin and fat are removed. 2. Incision is closed, and the skin heals with a scar. Illustration by You Jeong (Julie) Park, MD.
How it’s done: After the mastectomy, the surgeon removes excess skin and pockets of fat and tightens and smooths out the remaining tissue to create an even, flat chest. In some cases, the surgeon can use fat grafting (taking fat from another part of the body) or tissue transfer (taking tissue from another part of the body) to smooth out the shape. The fat or tissue fills out any divots or indentations and avoids a “scooped-out” look.
When it’s done: At the same time as the mastectomy, or later as a separate procedure. Some people get an aesthetic flat closure after they’ve had implant or flap reconstruction if they’re unhappy with the results or had complications.
Who can get it: Most people who are getting a mastectomy or have had one in the past can get aesthetic flat closure.
Length of surgery: 1 hour for one side or 2–3 hours for both sides
Oncoplastic surgery
Pros:
usually only tissue from the breast area is used (no implants or flaps)
many techniques can be used, and there are many options for cosmetic results; can include a breast lift and/or reduction
Cons:
longer surgery and recovery time than lumpectomy alone
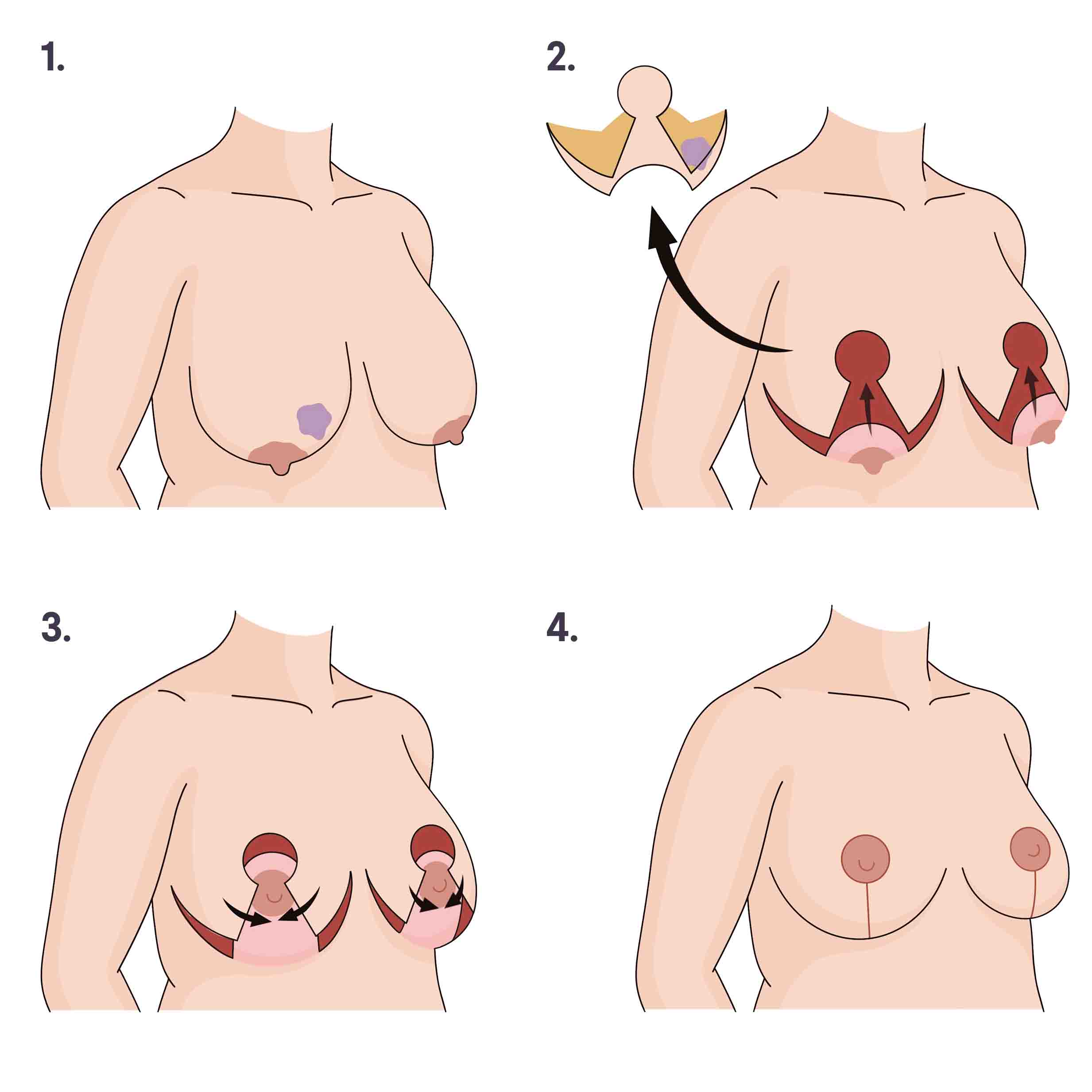
1. Breasts before surgery, with tumor (purple) in right breast. 2. Breast skin and tissue, including tumor, are removed. The nipples stay attached to the chest. 3. The nipples are repositioned higher, and the skin is redraped over. 4. Incisions are closed with nipples in their new position. Illustration by You Jeong (Julie) Park, MD.
How it’s done: After the lumpectomy, the surgeon reshapes the breast(s) using the tissue in the breast area. Many different techniques can be used in oncoplastic surgery. For example, the surgeon might rearrange breast tissue to fill in the area of tissue that was removed. In some cases, a breast implant, transplanted tissue flap, or fat grafting might be used in addition to the rearranged breast tissue to replace lost volume. In addition, the surgeon may perform a breast reduction or breast lift on the affected and unaffected breasts to make them more symmetrical. They may relocate nipples to make them more symmetrical. And they will also usually use techniques to prevent and reduce scarring.
When it’s done: Usually it’s done at the same time as the lumpectomy, right after the cancer is removed, but in some cases it can take place weeks, months, or years later.
Who can get it: Oncoplastic surgery tends to work best for people with moderate to large breasts. Sometimes people with smaller breasts can be candidates if the oncoplastic surgery will involve using an implant, flap, or fat grafting.
Length of surgery: 2–4 hours, depending on which techniques are used
Other Procedures
Many people opt for additional procedures to fine tune their results or fix a complication after breast reconstruction surgery.
Surgery to match the breasts
If you’re having a mastectomy or lumpectomy on one breast, you may have the option to have reconstruction surgery on the unaffected breast. This is sometimes done to make the breasts look more symmetrical.
Nipple Reconstruction
If your nipples were removed during a mastectomy, you may decide to reconstruct the nipples with surgery, tattoos, or both.
Breast Implant Removal
There are many procedures to correct a complication of breast reconstruction. For instance, if you develop capsular contracture or one of your implants ruptures, you might opt for breast implant removal (explant) surgery with or without additional reconstruction.
Talking with others who’ve had reconstruction
As you’re considering your options, it can be helpful to connect with people who’ve had different types of breast reconstruction — or no reconstruction. They can share their experiences, give you an idea of what to expect, or give feedback on plastic surgeons. You can connect with others who’ve had or are considering reconstruction in Breastcancer.org’s online message boards and virtual support groups.
This information made possible in part through the generous support of www.BreastCenter.com.