For Women in the Rural South, a Breast Cancer Diagnosis Often Comes Late
For some women, where you live can make the difference between an early cancer diagnosis and a late one.
A new study found that women living in the rural South are more likely to get a late-stage breast cancer diagnosis compared with women in other rural parts of the United States. And rural Black and Hispanic women, as well as women without insurance, have an even higher risk of a late-stage diagnosis (stage III or stage IV) compared to white women and those with insurance.
About 1 in 5 Americans live in rural areas in the country, which tend to be less crowded and away from big cities. But these communities face specific challenges that affect their health: They tend to have lower incomes and are more likely to be uninsured than people living in cities. They may also live far from doctors and hospitals, making it harder to get preventive cancer screenings and timely care.
It’s because of barriers like these that people living in rural America are more likely to get a late-stage cancer diagnosis and are less likely to survive than people in cities, according to the American Cancer Society. People in urban areas with better access to screening still get diagnoses, they just catch their cancer earlier, when it’s easier to treat. This latest research gives clues to how programs can address this divide.
The cancer impact in rural America
Omolade Sogade, MD, a surgery resident at Washington University-St. Louis, treats people from rural communities, many of whom travel to St. Louis for care. Sogade, who led the new study, wanted to better understand how cancer is diagnosed in rural communities across the country. So she dug into the data of more than 50,000 rural women with breast cancer from the National Cancer Database.
She found that it’s not just the rural-urban cancer divide that drives up late-stage breast diagnoses. Women in certain rural regions are far more likely to get a late diagnosis than women in other regions.
Women living along the Mississippi Delta — in parts of the rural South including Louisiana, Mississippi, and Arkansas — had the highest rates in the country. Women in this region were around 30% more likely to get a stage III or stage IV diagnosis than women in Iowa and the Dakotas. The New England region, including Vermont and Maine, had the lowest rates of stage III and IV diagnoses despite being one of the most rural parts of the US. This suggests it's not just rurality driving late diagnoses.
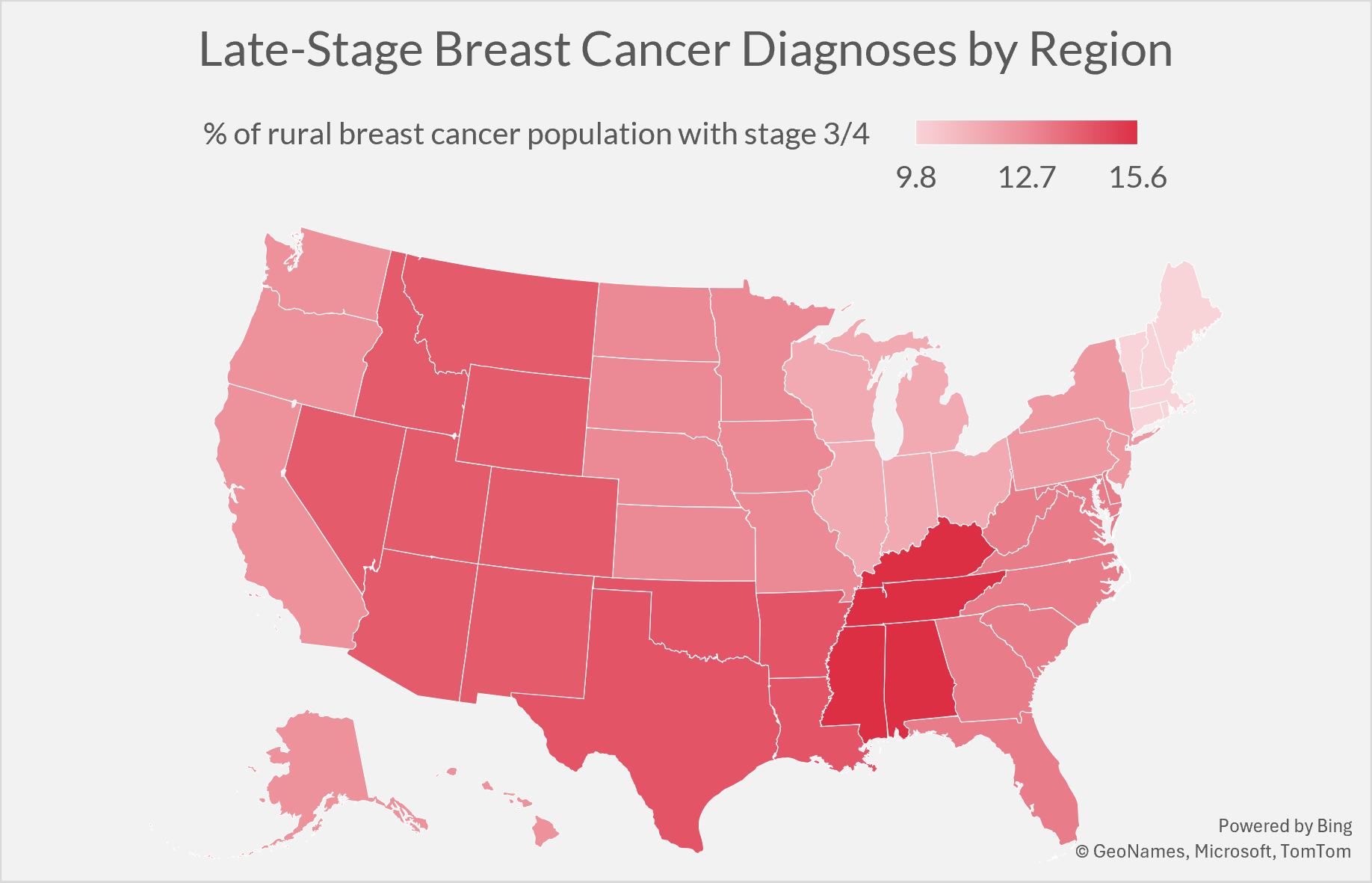
A map showing the percentage of breast cancer diagnoses in rural America that are stage 3 or stage 4. Percentages are by region, not by single state. New England (CT, MA, ME, NH, RI, VT), Middle Atlantic (NJ, NY, PA), South Atlantic (DC, DE, FL, GA, MD, NC, SC, VA, WV), East North Central (IL, IN, MI, OH, WI), East South Central (AL, KY, MS, TN), West North Central (IA, KS, MN, MO, ND, NE, SD), West South Central (AR, LA, OK, TX), Mountain (AZ, CO, ID, MT, NM, NV, UT, WY), Pacific (AK, CA, HI, OR, WA). Source: Sogade, O.O., & Margenthaler, J.A. J. Am. Coll. Surg. 2026, DOI: 10.1097/XCS.0000000000001759
Sogade looked at how race and ethnicity could affect when breast cancer gets diagnosed. She found that rural women were more likely to be diagnosed with late-stage breast cancer when they were Black or Hispanic. This tracks with Sogade’s regional findings: The Mississippi Delta, for example, has a majority Black population and is one of the poorest regions in the country, according to the U.S. Commission on Civil Rights.
Insurance also plays a big role. Women without insurance had a higher chance of getting a late-stage diagnosis than those with insurance. Medicaid helped lower that risk, but women on Medicaid still were more likely to be diagnosed late than women with private insurance. “And Medicaid is not evenly distributed across the country,” says Sogade. Alabama, Mississippi, and Tennessee are 3 of the 10 states that haven’t expanded Medicaid, meaning more people in these states are uninsured.
Sogade’s research shows that there’s likely not one reason for the rural-urban cancer divide, but rather causes that vary by region. She believes medical centers in areas with high rates of late-stage diagnoses should take a closer look at their communities. In the next phase of her research, Sogade hopes to learn what may be getting in the way of early detection for the people treated at WashU. “Maybe it’s inaccessible screenings, or not having transportation, time off of work, or childcare,” she says.
Reaching rural communities and closing the gap
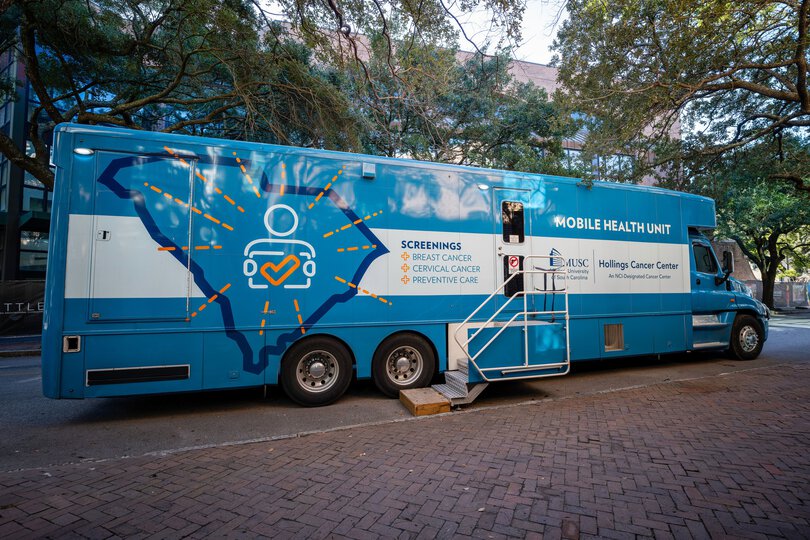
The mobile breast and cervical cancer screening truck from Medical University of South Carolina’s Hollings Cancer Center in Charleston, SC, provides 3D mammograms and breast exams to rural and urban communities. Photo courtesy of Rachel Smith.
Some medical centers and advocacy organizations are already doing what Sogade suggests: meeting the specific needs of their local communities. One approach involves sending mobile mammogram buses into communities so people don’t have to travel far for screenings.
And some states are expanding telehealth services and increasing the number of healthcare providers in rural areas. Right now, rural communities face a shortage of primary care doctors and only around 3% of oncologists practice in rural areas.
Sogade says multiple strategies will be needed to address the health gaps that rural communities face. She hopes research like hers will lead to regional health policies that provide transportation vouchers to help people travel to screenings or encourage companies to bring a mammogram bus to their worksites.
Tips for accessing breast cancer screenings
If you live in a rural area, there are several ways to access free or low-cost mammograms.
Check to see if you qualify for screenings through the CDC’s National Breast and Cervical Cancer Early Detection Program.
Find your local federally qualified health center, which may offer free and low-cost cancer screenings.
Apply to the American Breast Cancer Foundation’s Breast Cancer Assistance Program.