Breast Reconstruction Surgery With Implants
Breast reconstruction surgery with implants is one of the two main breast reconstruction surgery techniques. A breast implant is a round, flexible silicone shell filled with either saline (saltwater) or silicone gel. The implant replaces breast tissue that is removed during a mastectomy or lumpectomy, restoring the shape and volume of the breast.
If you're considering breast reconstruction, it can be helpful to meet with plastic surgeons before you have the mastectomy or lumpectomy. That way, they can talk you through your options. Individual plastic surgeons may have different levels of skill and experience, perform different types of procedures, and prefer different techniques. You want to feel comfortable with your surgeon’s experience and ability to clearly explain the advantages and disadvantages of your reconstruction surgery options.
Is breast reconstruction with implants right for you?
Breast reconstruction with implants may be a good option for you if:
you have enough healthy skin and tissue to cover and support a breast implant
you'd like to avoid the incisions and scars on other parts of your body that result from flap reconstruction
you prefer the shorter, less complex surgery with a shorter hospital stay and quicker recovery time than you’d need with flap reconstruction
you don't need radiation therapy (radiation often causes the skin over an implant to become tighter, tougher, and more rigid, and it can raise your risk of complications, such as infection around the implant)
About breast implants
Breast implants vary in:
size
shape
projection or profile (how much the implant projects forward from the chest wall)
filling type
surface texture
All breast implants have an outer shell made of silicone, a flexible, rubber-like material. You can choose whether the shell is filled with saline or silicone gel. The temperature of the saline or silicone can be different from your normal body temperature, especially in very cold or hot environments, and some people may notice these changes more than others. Your plastic surgeon can help you decide which implant is best for you and your body type.
Saline-filled breast implants
Saline-filled implants are filled with saltwater. The surgeon inserts the empty shell and, once it’s in place, fills it with saline until it’s the desired size.
Some people prefer saline-filled implants because:
if a saline implant gets a leak or rupture in its shell or its valve fails, it’s usually obvious because the saline leaks out and the breast appears deflated
saline is harmless and absorbed by the body
you don’t need to get routine MRI screenings to check for silent rupture (implant break that doesn’t cause any noticeable symptoms)
However, a disadvantage of saline implants is that some people think they feel less natural than silicone implants. Also, rippling and wrinkling on the surface of the implant is more likely to be visible through the skin.
Silicone-filled breast implants
Silicone-filled implants are pre-filled with silicone gel.
Some people prefer silicone-filled implants because:
they may look and feel softer and more like natural breast tissue than saline implants
the surgeon might be able to provide more brands and styles of implants to choose from (since more of the implants on the market are silicone-filled)
There are several disadvantages of silicone-filled implants, though, related to what happens if there is a rupture.
If a silicone-filled implant ruptures, it’s harder to recognize because the implant often maintains its shape. If the silicone gel comes out of the implant, it can stay in the body and may spread to nearby tissues or to other parts of the body such as the lymph nodes or the lungs.
Signs that your silicone-filled implant has ruptured can include changes in breast shape and size and increasing pain, firmness, and swelling over several weeks. The rupture of a silicone-filled implant can also cause capsular contracture (tightening of the scar tissue capsule around the implant).
Smooth versus textured breast implants
The outer silicone shell of a breast implant can be either smooth or textured. Implants with textured surfaces have been linked to a small increased risk of breast implant-associated anaplastic large cell lymphoma (BIA-ALCL), a rare type of T-cell lymphoma (cancer of the immune system).
Many plastic surgeons have stopped using textured implants and tissue expanders in recent years. But if you’re concerned about the risks linked to textured implants and tissue expanders, let your plastic surgeon know you prefer smooth-surfaced implants and tissue expanders.
What to expect with breast implant reconstruction surgery
Most people who have breast implant reconstruction have at least two surgeries over a six- to 12-month period:
In the first surgery, the surgeon places a tissue expander. The expander helps to create a space for the permanent breast implant. After this surgery, you’ll go for regular office visits weekly or biweekly for several months so that your plastic surgeon can gradually fill the expander with sterile saltwater or air until a desired size is reached.
In the second surgery the surgeon removes the tissue expander and replaces it with a breast implant.
You can have the first reconstruction surgery (in which the tissue expanders are placed) at the same time as mastectomy (called immediate reconstruction) or at a later date (delayed reconstruction). Some plastic surgeons think you can get better cosmetic results when implant reconstruction is done at the same time as mastectomy. Talk with your medical team about what’s best for your situation.
Sometimes it’s possible to have direct-to-implant breast reconstruction at the same time as mastectomy, meaning tissue expanders are not used.
Delayed reconstruction (that takes place in the months or years after a mastectomy) might be a better option for you if:
your skin is too tight to close over a tissue expander or implant
your skin doesn't have a good enough blood supply after the mastectomy
you need more time to decide which type of breast reconstruction you’d like to get
you need to receive certain other breast cancer treatments after the mastectomy (such as radiation therapy)
you have health problems that make it riskier to have a longer surgery — for example, uncontrolled diabetes, heart disease, or lung disease
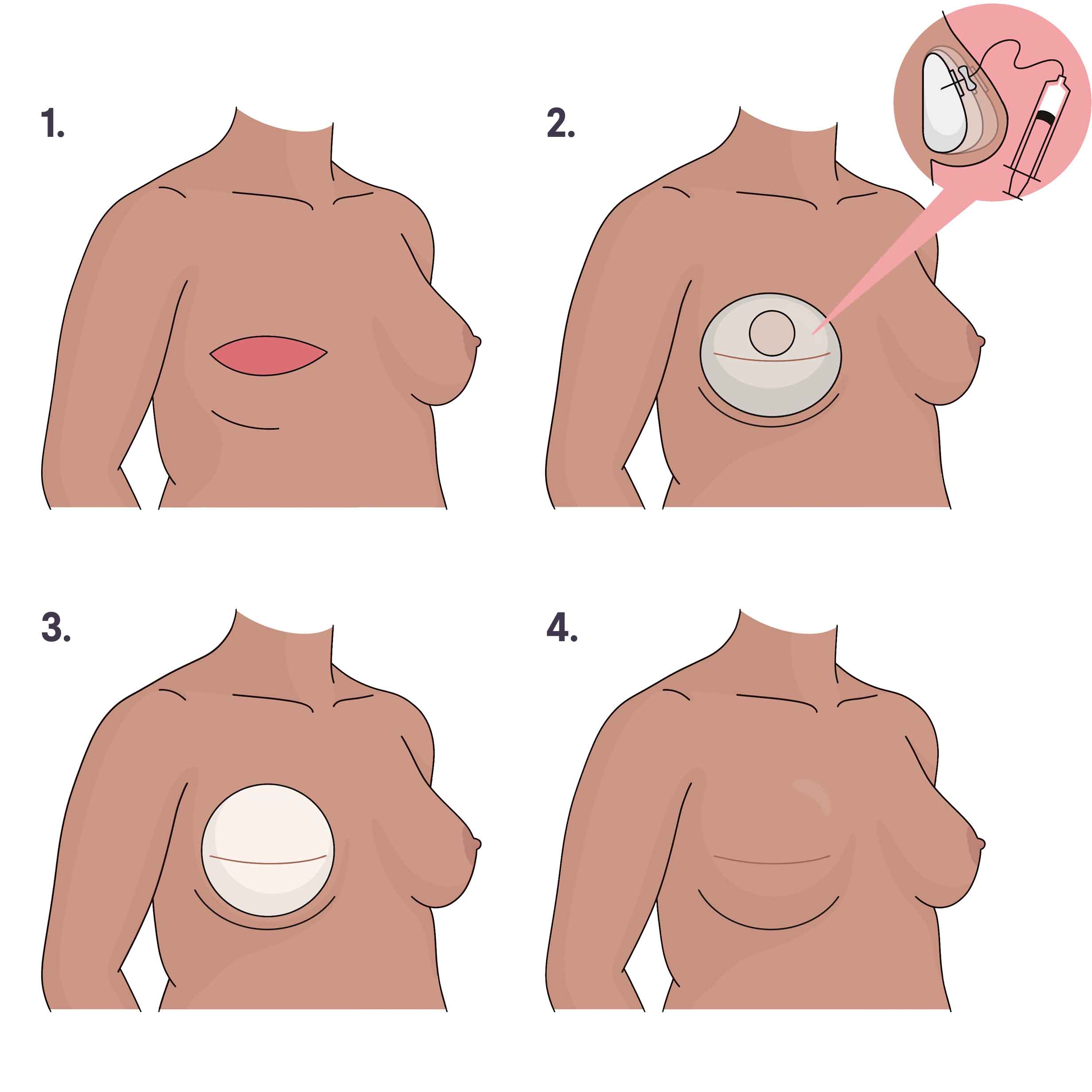
1. Breast tissue and nipple are removed. 2. A tissue expander is placed and gradually filled with sterile water over several weeks until it’s the preferred size. 3. The expander is exchanged for a permanent breast implant in a second surgery. 4. The breast, with implant, heals with a scar. Illustration by You Jeong (Julie) Park, MD.
About breast implant placement
Breast implants can be placed either underneath part or all of the chest muscle (subpectoral or under the muscle) or on top of the chest muscle (prepectoral or over the muscle). Talk with your surgical team to see which placement is best for you.
Depending on how the mastectomy goes, the surgical team might not be able to place the implant in the agreed-upon spot. For example, under-the-muscle placement may not be possible if some of the chest muscle is removed during mastectomy. Over-the-muscle placement may not be possible if the remaining breast skin is not thick or healthy enough after mastectomy.
Under-the-muscle or subpectoral placement
When the breast implant is placed underneath part or all of the chest muscle, surgeons usually cut or divide part of the chest muscle so they can place the implant underneath. Surgeons may sew a material called acellular dermal matrix (a soft tissue substitute made from human or animal skin) to the tissue at the bottom of the breast to create a pocket that helps to hold the lower half of the implant in place.
Advantages:
there is a lower risk of implant rippling or wrinkling because the chest muscle on top of the implant can help prevent its outlines from being visible through the skin
there is a lower risk of capsular contracture
Disadvantages:
there may be more discomfort during recovery from surgery and, in some cases, chronic pain, tightness, and weakness (because the chest muscle was cut, divided, or both during the procedure)
there is a higher risk of dynamic distortion (or animation deformity), which makes the breasts move in unnatural-looking ways when you flex your chest muscle
Over-the-muscle or prepectoral placement
Breast implants that are placed on top of the chest muscle directly under the skin don’t have as much soft tissue coverage as implants that are placed under the chest muscle. Surgeons may wrap the implant in acellular dermal matrix material and sew the material to the surrounding tissue. This helps support the implant, keeps it in place, and makes it less visible through the skin.
Your plastic surgeon can advise whether prepectoral implant placement is an option for you based on certain factors, including the amount and condition of the breast skin that remains after mastectomy. More plastic surgeons have experience with subpectoral implant placement, so it may be challenging to find a surgeon who can do prepectoral placement.
Advantages:
there is less pain, tightness, and weakness during and after recovery
there is a lower risk of animation deformity or dynamic distortion
Disadvantages:
there is a potential risk of implant rippling and wrinkling showing through the skin if the implant is not covered by enough soft tissue
there is a slightly higher risk of developing an infection around implants placed over the muscle than with implants placed under the muscle
there is a possible risk that the implant shifts out of the correct position over time if your breast skin is thin
Your surgeon may recommend one to three fat-grafting treatments sometime after implant reconstruction surgery to help thicken the soft tissue layer over the implant and prevent wrinkling and rippling.
Hybrid breast reconstruction
Hybrid breast reconstruction means the plastic surgeon uses a flap of your own tissue (from the belly, upper buttocks, or back) as well as a small breast implant to rebuild the breast. This approach may be recommended to people who don’t have enough body fat (in the area of the flap that will be used) to build a breast of the desired size. Learn more about hybrid breast reconstruction.
Breast implant follow-up care
Before having breast implant reconstruction surgery, it’s essential to understand the importance of follow-up care.
Breast implants don’t have a specific expiration date, but they don’t last a lifetime. It’s normal for people who have breast implant reconstruction to have one or more surgeries because of a complication or to improve how their breasts look and feel. The longer you have implants, the greater the risk that a complication might develop. Plastic surgeons often say that as a general guideline you should expect to get your implants removed and replaced about every 10 years.
You need a checkup once a year with a healthcare professional (such as a breast surgeon or plastic surgeon) who can check your implants for rupture and other problems. Of course, if you notice any abnormal changes in your breasts or implants, you need to see a healthcare provider right away.
Checking for breast implant rupture
The U.S. Food and Drug Administration (FDA) recommends that people with silicone-filled implants have routine imaging with ultrasound or MRI to screen for silent rupture. Screening for silent rupture should start five to six years after the implant is placed and then every two to three years afterward. Getting health insurance to cover these imaging tests can be challenging. Your plastic surgeon may be able to help you work with your health insurance company to get approved coverage for silent rupture screening in advance.
Ruptured silicone-filled implants have greater health risks than ruptured saline-filled implants and should be removed. When silicone gel leaks past the scar tissue capsule around the ruptured implant, plastic surgeons try to remove as much of it as they can.
Other potential complications after breast implant reconstruction
In addition to implant rupture, other possible complications of breast implant reconstruction surgery include:
capsular contracture: tightening of the scar tissue capsule around the implant
implant displacement: when the implant shifts away from its correct position in the breast
Breast implant illness (BII): a range of symptoms, such as joint and muscle pain, chronic fatigue, memory and concentration problems, that can develop after implant reconstruction
rare forms of cancer, including BIA-ALCL, other types of lymphomas, and squamous cell carcinoma
Learn more about breast implant reconstruction risks and complications.
Read Breastcancer.org’s Special Report: Breast Implant Illness and BIA-ALCL.
Preparing for breast implant reconstruction surgery
Your surgical team should review a patient decision checklist with you — to make sure you understand the risks and benefits of breast implant surgery — as required by the FDA. You and your surgeon should sign this checklist as part of the informed consent process.
Your surgical team will give you instructions on what to do before you have surgery (called pre-op instructions). These may include adjusting the medicine you take, not eating or drinking after a certain time, and showering with a special antibacterial skin cleanser.
You’ll also get instructions to follow after each surgery to help you as you recover (called post-op instructions). These instructions include recommendations for special exercises that minimize stiffness and scar buildup after immediate reconstruction, and how to care for the dressings, stitches, staples, and surgical drains.
Recovery from breast implant reconstruction surgery
It can take between six and eight weeks to recover from surgery. Take the time you need to heal, continue doing your exercises every day, and follow any other instructions your surgical team or physical therapist prescribes for you.
If you had surgery for tissue expanders first, the second surgery to remove the expanders and replace them with breast implants is usually scheduled two to six months later. This follow-up surgery is usually an outpatient procedure, which means you don’t stay overnight in the hospital.
After breast implant reconstruction
Once your reconstructed breasts have healed and settled into a final position — about four to six months after your final breast implant reconstruction surgery — you might decide to have other procedures to improve the results. For example:
nipple tattoos, nipple reconstruction surgery, or both
fat grafting, which can be used to fill in imperfections or add volume to the reconstructed breast, soften and improve skin affected by radiation therapy, and thicken the layer of tissue between an implant and the skin
corrective surgery to make scars from breast surgeries less visible, to correct asymmetry, or to address a complication that might have resulted from breast implant reconstruction surgery
Breast implant reconstruction images

Before and after bilateral skin-sparing mastectomy and direct-to-implant breast reconstruction.

Double mastectomy and reconstruction with implants and nipple tattooing.

This information made possible in part through the generous support of www.BreastCenter.com.